
Percutaneous Coronary Intervention (PCI): Angioplasty & Stent
The coronary arteries are the vessels that supply the heart muscle with oxygen. When atherosclerotic plaques narrow or block them, the heart receives less blood and the consequences can range from chest pain to a full-blown heart attack. Until recently, coronary artery bypass grafting (CABG) was often the only option. Today, percutaneous coronary intervention (PCI) restores blood flow without opening the chest, in a matter of minutes, under local anaesthesia.
What is coronary artery disease?
Coronary artery disease develops gradually as fatty deposits and calcium accumulate within the arterial wall, forming atherosclerotic plaques. The vessel's opening narrows, blood flow is restricted, and the heart muscle no longer receives enough oxygen.
The most common symptoms include:
- Chest pain or tightness (angina), typically triggered by physical exertion
- Shortness of breath during activity or at rest
- A sense of pressure or heaviness in the left shoulder blade or jaw
- Unexplained fatigue and dizziness
- In the most severe form: acute myocardial infarction (heart attack)
What is PCI (Percutaneous Coronary Intervention)?
PCI (Percutaneous Coronary Intervention) is a minimally invasive procedure that opens narrowed or blocked coronary arteries using a thin, flexible catheter, with no incision in the chest and no need for cardiopulmonary bypass. The goal is straightforward: to restore normal blood flow to the heart muscle.
How is the procedure performed step by step?
- Access: The interventional cardiologist introduces a thin catheter, usually through the radial artery at the wrist (radial approach) or the femoral artery at the groin
- Guidance: Using fluoroscopy and contrast dye, the catheter is navigated precisely to the affected coronary artery
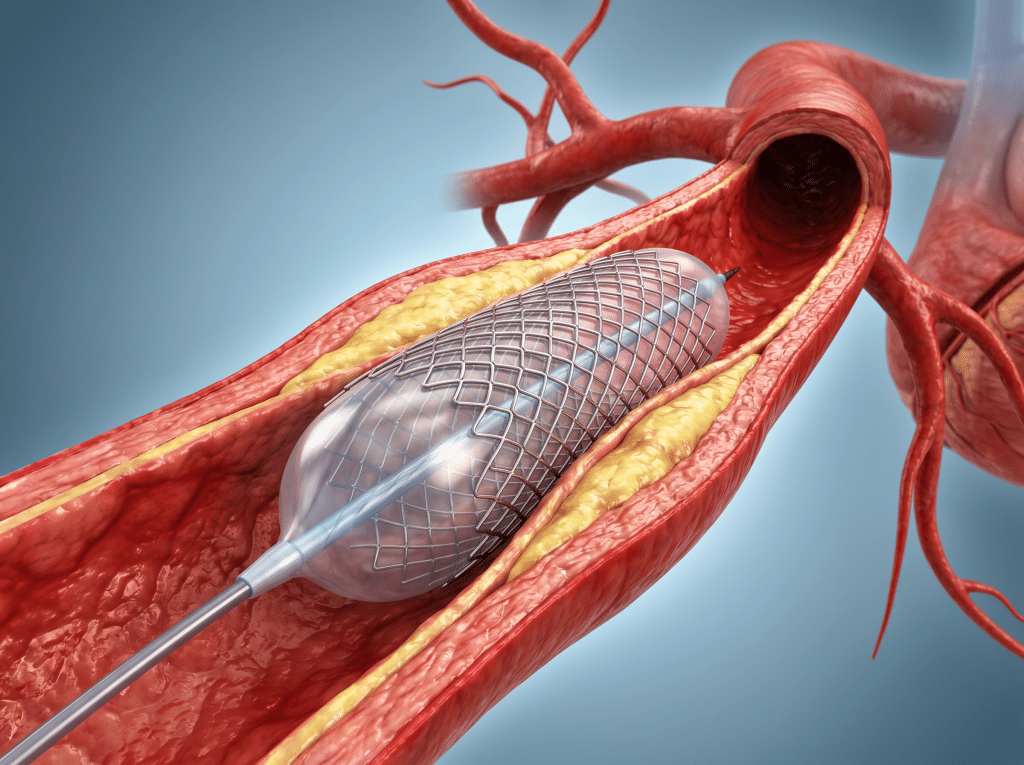
- Dilation: A small balloon is inflated at the site of the blockage, compressing the atherosclerotic plaque against the vessel wall
- Stenting:: In the vast majority of cases, a stent, a metal mesh scaffold, is deployed simultaneously to support the artery and keep it open
Types of stent: what we choose and why
Stent selection is based on the anatomy of the lesion, the presence of diabetes, and other clinical factors. The two main options today are:
- Drug-Eluting Stents (DES): The gold standard of modern PCI. These stents gradually release antiproliferative agents that prevent restenosis (re-narrowing of the artery). They account for over 80% of stents implanted worldwide.
- Bioresorbable Scaffolds (BRS): These provide structural support during the healing phase and are gradually absorbed by the body within 1–3 years, allowing the artery to recover its natural function. Research in this area remains highly active.
When is PCI indicated?
Dr. Kolyviras evaluates each case individually, based on clinical findings, coronary angiography results, and the guidelines of the European Society of Cardiology. PCI is the treatment of choice in:
- Acute ST-elevation myocardial infarction (STEMI): Primary PCI is the first-line emergency treatment
- Unstable angina / NSTEMI: Early intervention to prevent a further ischaemic event
- Stable coronary artery disease with persistent symptoms despite optimal medical therapy
- Confirmed significant ischaemia on functional testing (exercise stress test, coronary FFR)
Why choose PCI over bypass surgery?
PCI is not the right answer for everyone. In patients with multi-vessel disease or left main coronary artery disease, bypass surgery may offer better long-term outcomes. For the majority of patients, however, PCI carries clear advantages:
- No general anaesthesia or sternotomy: The procedure is performed under local anaesthesia
- Rapid recovery: Most patients return home within 24–48 hours
- Immediate symptom relief: Reduction in angina and breathlessness is typically felt from the very next day
- Safe even for elderly patients and those at high surgical risk due to comorbidities
Expertise and Care at Metropolitan General
Every case of coronary artery disease is unique. At Metropolitan General, Dr. Thanos Kolyviras uses advanced intraoperative imaging, including intravascular ultrasound (IVUS) and fractional flow reserve (FFR), to plan and guide each PCI with precision, ensuring the best possible outcome for every patient.
Restoring coronary blood flow is not simply a technical procedure, it is a return to daily life, free from fear and free from pain. We are here to assess your condition and discuss whether PCI is the right choice for you.
Συχνές Ερωτήσεις
How long does a PCI procedure take?
The procedure is typically completed in 30–90 minutes, depending on the number and complexity of the lesions. The patient remains conscious throughout.
Is hospitalisation required after PCI?
For elective (planned) procedures, patients are usually discharged within 24–48 hours. In emergency cases such as STEMI, the hospital stay may be slightly longer for monitoring.
What medications are needed after stent placement?
Following PCI, dual antiplatelet therapy, typically a combination of aspirin and a second antiplatelet agent, is required for several months or years, depending on the stent type and the patient's overall health. Strict adherence to this treatment is critical.
Could a repeat procedure be needed in the future?
With current-generation drug-eluting stents, the restenosis rate has fallen below 5–10%. Regular follow-up with the interventional cardiologist, combined with ongoing medical therapy, reduces this risk further.
Is PCI appropriate for elderly patients?
Yes. The absence of general anaesthesia and cardiopulmonary bypass makes PCI particularly well suited to elderly patients or those with comorbidities that would make open surgery high-risk.